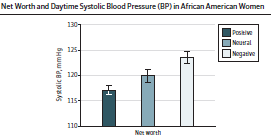
hypertension: net worth as risk factor in African-American women
A recent study found a significant relationship
between negative net worth (ie, debt) and higher blood pressure in
African-American women, controlling for some of the other measures of social
economic status including educational level and family income (see htn
networth assoc BP in AfAm women jama2022 in dropbox
or doi:10.1001/jamanetworkopen.2022.0331)
Details:
--384 African-American women were enrolled in
the Mechanisms Underlying the Impact of Stress and Emotions on African American
Women's Health cohort who participated in the study, from 2016 to 2019
--all were aged 30 to 45 at screening, were
premenopausal, and were not pregnant/lactating
--exclusion criteria included a history of
clinical cardiovascular disease, illnesses that might influence CVD risk (eg,
autoimmune disease, HIV, kidney disease), psychiatric disorder treatment,
illicit drug use, or shift-working (owing to alterations in circadian rhythm)
--50% of the participants by design were above
and 50% below the median income of $50,000 in Georgia at the time of their
recruitment
--mean age 38, educational level overall less
than college 29%/some college 22%/finished at least college 49%), income
overall 25% had <$35,000, 21% $35,000-$50,000, 22% $50,000-$75,000, 32%
>$75,000 in this highest income group; current smoker 10% versus; 39%
were married or had a live-in partner
-- positive net worth was reported
in 48% and negative net worth in 29% (23% had neutral net worth)
-- comparing those with positive
versus negative net worth: income >$75,000 in 47% versus 16%, college
graduates in 59% versus 42%, being married/living with a partner 46% versus
28%, lower BMI 8% versus 9%, less likely to smoke 6% versus 16%, less
likely to report debt stress 4% versus 6%, less likely to have depressive
symptoms 4% versus 8%
--48-hour ambulatory blood pressure monitoring
(ABPM) was performed, as well as initial in-person visits in which height,
weight, two seated measures of resting blood pressure, and additional clinical
information was assessed
-- net worth was assessed by asking:
"suppose you and others in your household were to sell all of your major
possessions (including your home), turn all of your investments and other
assets into cash, and pay off all of your debts. Would you have something left
over, break even, or be in debt?", a question asked in prior research
studies
--Main outcome: mean daytime and nighttime blood
pressure levels, assessed by 48-hour ambulatory blood pressure monitoring
(ABPM), and sustained hypertension (ABP daytime and clinic BP>130/80 mmHg)
--linear regression models were adjusted for
age, marital status, educational level, family income, and family size
Results:
--Ambulatory blood pressure readings, comparing
positive versus negative net worth groups:
-- daytime systolic blood
pressure: 119 mmHg (SD 12 mmHg) versus 124 mmHg
(SD 12mmHg), p<0.001
-- nighttime systolic blood pressure: 109 mmHg (SD 11 mmHg)
versus115 mmHg (SD 12 mmHg), p<0.001
-- daytime diastolic blood pressure: 76 mmHg
(8 mmHg) versus 79 mmHg (SD 8mmHg),p=0.01
-- nighttime diastolic blood pressure 67 mmHg
(SD eight mmHg), versus 71 mmHg (SD nine mmHg),
p=0.002
--
sustained hypertension: 25% in those with positive net worth versus 40% in
those with negative net worth, p=0.02
--Antihypertensive use was not significantly different between debt groups, 17%
-- debt
stress: 3.6 (standard deviation, SD 3) versus 5.6 (SD 3), p<0.001
-- depressive
symptoms: 4.4 (SD 5) versus 7.6 (SD 8), p<0.001
-- comparing women reporting a negative net
worth to those with a positive net worth, controlling for age, marital status,
educational level, family income, and family size:
--higher levels of daytime and
nighttime systolic blood pressure, both with p<0.001
--sustained hypertension: OR 2.5
(1.3-4.7)
-- these associations remained significant after
adjusting for smoking, BMI, psychosocial stress due to debt, and depressive
symptoms
-- results were attenuated slightly when the 66
women who were on anti-hypertensive medications were included in the analysis
(the above numbers excluded them)
Commentary:
-- net worth may well be a very important marker
of SES, since it does reflect long-term financial stability and economic
reserve. and this study suggested it might well be a much more sensitive marker
than some of the other surrogate markers of SES, such as education or family
income in this study. a couple of other studies have found that housing
instability (see https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3665966/,
though in this study was only found in white women), negative social
interactions (see https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4182094/),
or other social factors (see https://www.researchgate.net/profile/William-Dressler/publication/281870723_Dressler_William_W_1996_Hypertension_in_the_African_American_community_social_psychological_and_cultural_determinants_Seminars_in_Nephrology_16_71-82/links/55fc885608aeafc8ac495615/Dressler-William-W-1996-Hypertension-in-the-African-American-community-social-psychological-and-cultural-determinants-Seminars-in-Nephrology-16-71-82.pdf ).
there was a study i saw many decades ago (sorry, cannot find it) finding that a
social insecurity index, a combination of largely neighborhood stressors (do
you feel safe in your neighborhood? and several questions about people's
feelings about their living situation, crime, and generally whether they felt
their neighborhood was "desirable") largely negated any racial
differences in hypertension. newer studies reinforced this conclusion: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-016-3741-2
-- It was notable in the study
that net worth categories stratified all of the income levels as well as educational
levels of these women, and that net worth itself was significantly associated
with hypertension when controlling for these other socioeconomic factors
-- ambulatory blood pressure is the most
sensitive marker of future clinical events and is considered the gold standard;
it is the current recommendation of the USPSTF and several European health
agencies (eg NICE in UK). for many studies documenting the superiority of ABP,
see http://gmodestmedblogs.blogspot.com/search?q=ambulatory+blood )
--Though we do not have multiple measures of
blood pressure over time, it was clear from the study that in terms of
important socioeconomic variables to assess for middle-aged African-American
women, net worth was clearly superior to income or educational status.
-- Net worth is influenced by a number of
factors, all of which are much more deficient in African-American women:
-- racism (and the constant daily
stress associated), lower likelihood of dual earner partnerships, less likely
to achieve higher wage jobs independent of educational status (and wage
differentials between men/women, white/nonwhite), redlining of properties,
decreased access to many colleges and universities, and generally decreased
ability to achieve upward mobility and wealth
-- also, a big issue is inherited
wealth, so important for many people in our society, is very limited in the
African-American community
-- in 2016 dollars: white vs Black
income median $61K vs $35K; networth $171K vs 18K, per https://www.visualcapitalist.com/racial-wealth-gap/
Limitations:
-- much of the information was self-report,
including net worth, educational level, and income. The accuracy of these
assessments may be limited without objective data
-- we do not know what the blood pressure level
or control was at start of the study,. Nor the access to health care, ability
to afford medications
--this study provided an association between net
worth and elevated blood pressure, and therefore cannot determine a causal
relationship.
-- negative debt is a very low bar for this
association. there are many people who do have some assets or are living in a
situation that allows them to survive with a small surplus who would not be
classified as having negative debt
--
hypertension is an intermediate marker for clinical events, be they
cardiovascular disease, renal disease, strokes, atrial fibrillation, etc. But,
though the association is strong, this study did not assess actual clinical
endpoints (which is what really matters)
so, the real relevance of this study to me is:
--some of our quick and dirty assessments of
socioeconomic status (e.g. income, education level) may be quite inadequate
measures of the potentially adverse health and comes associated with lower SES
-- this study further lays bare that
social/economic inequities are associated with significant health
consequences in our society: it is pretty shocking in the richest country in
the world that lower income people live in debt and, associated with that, poor
health outcomes. especially at a time when income inequalities are accelerating
so rapidly. and, there are so many factors as noted above (racism, higher cost
of living in inner city/rural communities, housing/food insecurity, wage
differentials, generational inequalities, stress,...
.
so, there are a few take-aways from this study
-- it reinforces the well-accepted
understanding that social inequities are associated with poor health outcomes
-- in terms of assessing social
inequities, this study argues strongly that some of the easy-to-measure markers
(income, education) may be inadequate, and that networth may be much more
strongly associated with clinical outcomes.
-- and, this opens the arena
further: is hypertension/cardiovascular disease/peptic ulcer
disease/uncontrolled diabetes related to other aspects of social inequities
such stress, or feeling safe in one's community, or food/housing insecurity, or
racism, or single parenthood, or personal violence, or... (not that these
issues are only in poorer communities, but may be more frequently occurring
there)
geoff
If you would like to be on the regular email list
for upcoming blogs, please contact me at gmodest@uphams.org
to get access to all of the blogs (2 options):
1. go to http://gmodestmedblogs.blogspot.com/ to see them in reverse chronological order
2. click on 3 parallel lines top left, if you
want to see blogs by category, then click on "labels" and choose a
category
3. or you can just click on the magnifying
glass on top right, then type in a name in the search box and get all the
blogs with that name in them
or: go to https://www.bucommunitymedicine.org/ ,
a website from the Community Medicine section at Boston Medical Center.
This site does have a very searchable and accessible list of my blogs (though
there have been a few that did not upload over the last year or two). but
overall it is much easier to view blogs and displays more at a time.
please feel free to circulate this to others.
also, if you send me their emails, i can add them to the list

Comments
Post a Comment
if you would like to receive the near-daily emails regularly, please email me at gmodest@uphams.org